
Assessment
of Vascular Disease
History and Examination
The initial assessment of a patient is the most important part of the management of any patient. It is at this assessment that a mutual trust should develop between surgeon and patient. The assessment needs to be tailored to the presenting problem, but should be detailed enough to understand the full situation of each individual. Patients deserve a period of undistracted thought, concentrated on their particular problem. This is absolutely crucial in subsequent management, when often extremely important decisions are being made which can affect the subsequent life and limb of the patient. In modern busy hospitals this can be difficult with constant interruptions from the ubiquitous mobile phone. There is also a tendency in modern medicine to rely on blood tests and radiology imaging to provide a diagnostic answer. Although they provide important complementary information to the doctor, in isolation they are largely useless. All test results must be correlated with the clinical impression and provisional diagnosis gained from a careful history and examination. If there is a discrepancy between the clinical impression and the test findings the doctor needs to think again and at least try to provide a reasonable explanation as to why this discrepancy might be present.
The first part of the assessment of any patient, with any problem, is taking a detailed medical history and performing a physical examination. The time taken to do this initial assessment will depend on the presenting problem.
History
Arterial
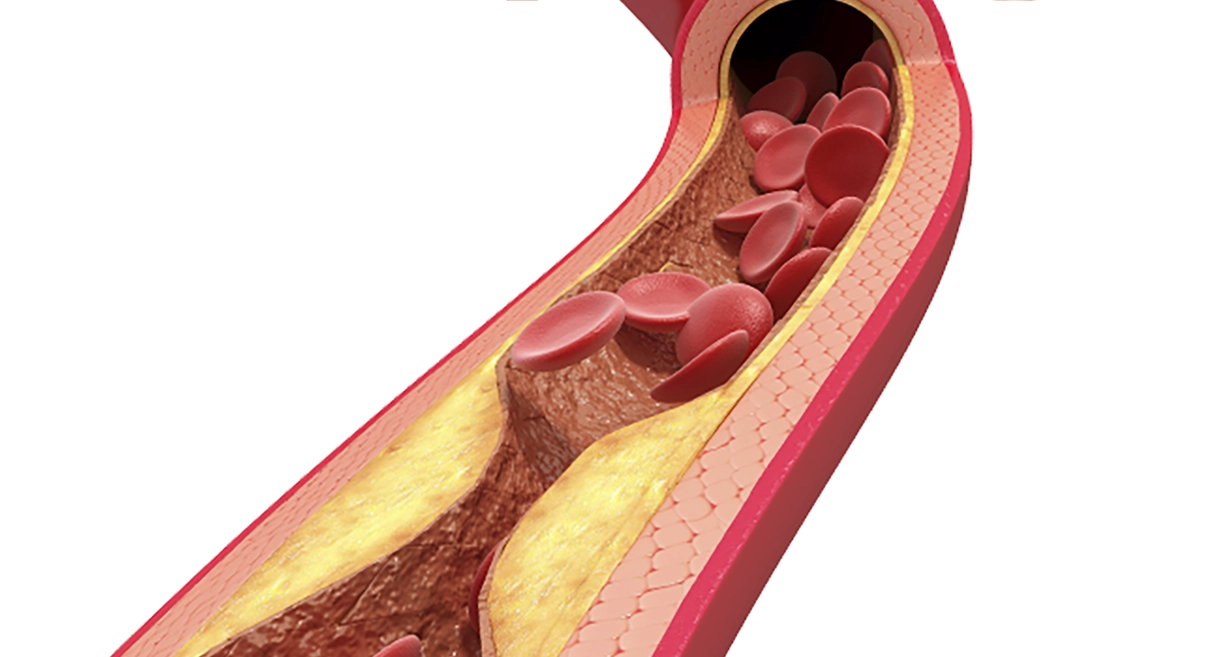
When a patient develops symptoms of pain in the leg due to arterial disease there are certain typical features. The pain is typically brought on by exercise and relieved by rest (claudication). Sometimes these features are not clear cut and close questioning by your vascular surgeon will be required to try to decide if your symptoms could be related to vascular disease. Sometimes it is more clear cut that arterial disease is present. The presence of gangrene or severe, unremitting pain in the foot at rest, are good indicators of more severe vascular disease.
Pain that is intermittently present in the foot or leg and occurs with exercise, but is also present at rest, is frequently not related to arterial disease. Other common causes are arthritis or nerve problems (neuropathy).
If you are seeing your surgeon because of a previous stroke or ministroke then your surgeon will want more detail on that stroke and exactly how it affected you. This is important because the decision to proceed with intervention or not will depend on these symptoms. Weakness on one side of the body lasting for more than one hour is significant when considering carotid endarterectomy. Dizziness however is a common symptom which is not usually related to carotid artery disease.
Aneurysms do not often cause symptoms, but your surgeon will often ask about back and abdominal pain, which can be a sign of impending trouble.
General vascular history includes asking about previous heart attacks and angina, current medication and general fitness particularly with regard to respiratory problems. This is important because many older people with arterial disease have serious co-existing disease which may influence future decisions about treatment. A detailed list of curent medications is essential. Warfarin is especially important as this usually must be stopped before any vascular intervention.
Venous
For patients with varicose veins or chronic venous insufficiency, your surgeon will want to know how long varicose veins have been present. The symptoms caused by your varicose veins will be important. It is important that the aching and discomfort in the legs is due to the veins, if you are to have treatment for your veins. Sometimes leg discomfort can be due to arthritis in the knees even when varicose veins are present. It is important to clarify the exact nature of the symptoms at an early stage so the true benefits of treatment can be assessed. Previous history of deep venous thrombosis, leg ulcers and broken bones in the leg can be important.
In patients with leg ulcers it is important to know how long they have been present and how they started. A previous history of leg ulcers can be important.
Lymphatic
The duration of swelling in the leg(s) and problems it has caused are important. Infection is the commonest problem. Any previous surgery and/or radiotherapy to the limb is important. Surgery in the armpit or groin may be particularly important in patients with lymphoedema.
Examination
Examination mainly comprises looking (inspection) and feeling (palpation). Tapping (percussion) and listening (auscultation) are also examination tools that can be helpful, but less so in vascular disease.
A full arterial examination can involve examining the hands or fingers for signs of smoking and raised cholesterol in the blood. The pulses in the arms will be compared and blood pressure measured in both arms. Raised cholesterol can also cause a white ring to appear around the iris (arcus). In the neck turbulent blood flow can produce a sound (bruit) that can be heard with a stethoscope. A bruit, however, is not a reliable indicator of underlying vascular disease in the carotid arteries in the neck.
In the abdomen an aneurysm can sometimes be felt, although this can vary enormously depending on the size of the patient and feeling is a poor way to detect an aneurysm or assess its size.
In the legs the appearance of the skin of the leg and foot may be helpful. The foot may blanch on elevation and become red and congested looking on dependency (Buerger’s sign). Gangrene and the presence of ulceration are concerning in the presence of arterial disease. The temperature of the skin and the presence of pulses in the leg and foot should be assessed.
The health of the skin is important in lymphoedema. It can frequently become thickened and scaly. Lymphoedema is often confined to the leg with relative sparing of the foot.
In venous disease the shape and colour of the leg are important. Pigmentation, eczema, swelling and ulceration are important signs of complications in venous disease. The distribution and size of varicose veins are recorded. The major venous junctions at the groin and behind the knee will be examined.
Blood tests
No blood test can be used to diagnose arterial or venous disease, but blood tests may assist in providing extra information. For instance the blood sugar level can determine if undiagnosed diabetes is present. The cholesterol level can be monitored and kidney function assessed. The full blood count will tell the surgeon whether you are anaemic or occasionally if there are too many blood cells present (polycythaemia).
Less commonly performed tests may be important in certain circumstances. Tests that assess the tendency to form blood clots (thrombophilia) and homocysteine levels can be useful because treatments are available to help these problems. In microvascular disease a vasculitic screen to assess the presence of destructive antibodies causing blood vessel inflammation (vasculitis) is used. D-dimer can be useful in the diagnosis of deep venous thrombosis.
Hand held Doppler
The hand held Doppler is an instrument that detects blood flow using the principles of the Doppler effect. It can be a very useful tool in assessing how good the blood flow is to the foot or hand. It is a painless test and very similar to taking blood pressure using a stethoscope. It is particularly useful for assessment of arterial disease but can also be used for venous problems. It is also commonly used to listen to the heartbeat of a baby in the womb and is completely harmless.

Using the Doppler, the blood pressure can be measured in the arm and the leg to assess whether any differences are present. Usually the blood pressure in the arm and the leg are the same and in these circumstances the ankle:brachial index (ABI) will be close to 1.0. For example a pressure of 120mmHg at the ankle divided by a pressure of 120mmHHg in the arm (brachial pressure) will give a ratio of exactly 1. If there is arterial disease in the leg then the blood pressure may be lower in the leg (for example 60mmHg pressure ) than in the arm (120mm Hg pressure) and the ABI will be less than 1.0, in this example 0.5 (60 ÷ 120).
Doppler measurements can also be performed before and after exercise. The leg pressure will decrease further in patients after exercise if there is atherosclerosis present.
Listening to the type of sound produced by the arterial flow is also useful. In normal patients the arterial signal has three phases (triphasic), but in the presence of arterial disease this signal becomes monophasic (one phase). Interpretation of the sounds is of particular benefit in patients when there is difficulty in measuring the pressures, such as in some patients with diabetes and renal failure.
The ABI and hand held doppler give the surgeon a more objective assessment of the severity of the arterial problem. It does not indicate to the surgeon whether treatment is required and is only complementary to the findings from the history and examination.
Duplex ultrasound

Ultrasound scanning has become one of the most important investigations used in the assessment of vascular disease. This is because it provides accurate information on the flow of blood in the arteries and veins, but it is painless and risk free. Ultrasound has been used safely for years to assess babies in the womb. The picture on the left shows a modern ultrasound scanner.
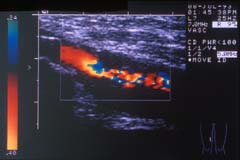
Colour flow ultrasound provides accurate information on most arteries. It can assess the flow of blood and whether there is any impairment of flow caused by hardening of the arteries. It is commonly used to assess aortic aneurysms, carotid arteries and the arteries to the legs as in the image (opposite) which demonstrates a narrowing of an artery in the thigh. It is especially useful in the assessment of venous disease as it can identify the sites in the veins leading to reflux (reverse flow).
Ultrasound requires a skilled operator to produce the most accurate information. In some circumstancesthe information obtained from Duplex scanning may be sufficient to make a decision on treatment. This is especially so for carotid surgery but I personally prefer some other supportive imaging before embarking on surgery.
Intra-arterial Angiogram

An angiogram (digital subtraction angiogram or DSA) produces a road map of the blood vessels. It is a good way of examining the anatomy of the blood vessels and tells the surgeon which blood vessels are open and which are diseased, narrowed (stenosed) or blocked. More information is available by clicking here. Angiography is the most commonly used method of assessing the arteries before surgery.
It has one major disadvantage compared with the other techniques because it requires the placement of a needle inside the artery. This can be uncomfortable, but it is the only method of assessment, which can also be used to treat arterial disease by angioplasty. In addition angiography is the gold standard investigation in determining whether arterial narrowing or occlusion is present.
Magnetic resonance angiography

Magnetic resonance angiography (MRI and MRA) is one of the newer techniques whic also provide a road map of the arteries. It is a technically complicated imaging method which relies on powerful magnets to align water molecules in the body tissues. It is a painless and fairly rapid form of assessment especially on the latest machines, but is noisy and some patients feel hemmed in or claustrophobic by the procedure.

It can be used to assess almost any artery in the body but has been found particularly useful in the assessment of carotid artery disease, as shown on the right. It is also good for assessing the renal (kidney) arteries. It does not require puncture of an artery and consequently is only useful in the diagnosis of disease and cannot be used to treat arterial problems.
MRA is becoming an increasingly popular imaging technique for blood vessels. Some recent reports indicate there is a risk of kidney damage in some patients from the use of a gadolinium contrast medium.
CT (computed tomography) angiography

This test uses X-rays to produce horizontal cross-sectional images through the body which are then reconstructed using computers to produce longitudinal and 3-D images and so provide a detailed raod map of the arteries. The advantage of CT is that it does not require a puncture of an artery. If an angioplasty is required then this must be performed separately using conventional angiography.
CT angiography is also becoming more popular as 64 slice CT scanners become more prevalent. In the right hands CT angiography is probably as accurate as conventional angiography. Newer imaging suites are able to combine cross-sectional CT images with angiography in 3 dimensions.
CT also has risks of causing kidney damage from the use of a contrast medium in patients with already impaired kidney function.